Portal Hypertension: Managing Varices, Ascites, and Life-Threatening Complications
 Mar, 7 2026
Mar, 7 2026
When your liver is damaged, especially from cirrhosis, blood doesn’t flow through it the way it should. The pressure in the portal vein - the main blood vessel carrying blood from your intestines to your liver - starts to climb. This is portal hypertension. It’s not a disease on its own. It’s a warning sign. And left unchecked, it leads to dangerous complications like bleeding varices, fluid buildup in the belly (ascites), and even brain fog or kidney failure. If you or someone you care about has cirrhosis, understanding what happens next isn’t optional - it’s life-saving.
What Exactly Is Portal Hypertension?
Normal pressure in the portal vein is between 5 and 10 mmHg. When it pushes above 10 mmHg - or when the difference between portal and liver vein pressure (called the hepatic venous pressure gradient, or HVPG) hits 5 mmHg or more - you’re in portal hypertension territory. The American Association for the Study of Liver Diseases (AASLD) says this threshold is the clinical line. About 90% of cases come from cirrhosis. The rest? Non-cirrhotic causes like blood clots in the portal vein or rare liver conditions.
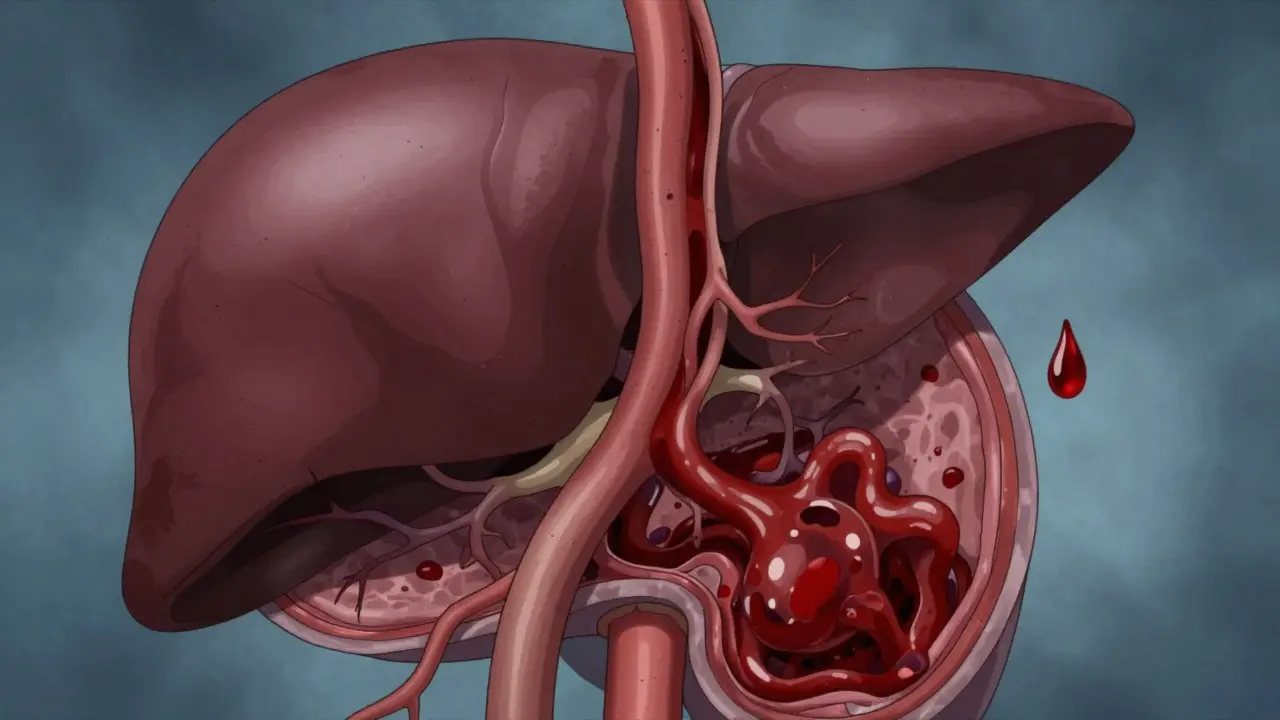
The real problem? Your liver is scarred. It’s stiff. Blood can’t squeeze through easily. So pressure builds. And then your body tries to compensate: blood vessels in your spleen and intestines widen, letting more blood rush toward the liver. But the liver can’t handle it. The extra flow just makes the pressure worse. This cycle keeps going. And over time, blood finds new paths - weak, swollen veins that shouldn’t be there.
Varices: The Silent Time Bomb
Half of all cirrhosis patients will develop varices - enlarged, twisted veins - in their esophagus or stomach within 10 years. These aren’t just swollen veins. They’re fragile. Like overinflated balloons made of thin tissue. A small bump, a cough, or even nothing at all can make them rupture. When that happens, you vomit bright red blood. Or pass black, tarry stools. It’s terrifying. And deadly. About 1 in 5 people who bleed from varices die within six weeks.
Doctors don’t wait for bleeding to happen. They screen. Endoscopy is the gold standard. If medium or large varices are found, treatment starts immediately. The go-to move? Non-selective beta-blockers like propranolol. Take enough to lower your resting heart rate by 25%. That’s the target. Studies show this cuts the risk of first bleeding by nearly half. But it’s not perfect. Side effects? Fatigue, dizziness, low blood pressure. Some patients can’t tolerate it.
For those with high-risk varices, or after a bleed, endoscopic band ligation is the next step. Tiny rubber bands are placed around the varices during an endoscopy. This cuts off the blood supply. It’s effective. Rebleeding drops from 60% to under 30%. But you need multiple sessions. And it’s not a cure. Varices can come back. That’s why long-term management is non-negotiable.
Ascites: When Your Belly Swells Beyond Recognition
Ascites - fluid leaking into your belly - affects 60% of cirrhosis patients within 10 years. It’s not just a cosmetic issue. It’s painful. Breathing gets hard. You can’t eat because your stomach feels full. Walking becomes a chore. And if it gets too tight, doctors have to drain it - a procedure called paracentesis. Remove 4 to 6 liters at a time. But every liter removed? You lose protein. That’s why albumin - a blood protein - is given intravenously. Six to eight grams per liter removed. It keeps your blood pressure stable and prevents kidney damage.
Before drainage, you start with diet and drugs. Sodium under 2,000 mg a day. That’s no processed food, no canned soups, no soy sauce. Spironolactone (100 mg daily) and furosemide (40 mg daily) are the go-to diuretics. Together, they work. About 95% of patients with simple ascites respond. But 10%? Their fluid won’t budge. That’s refractory ascites. And it’s serious. It often means your liver is failing. At that point, options shrink: TIPS or transplant.
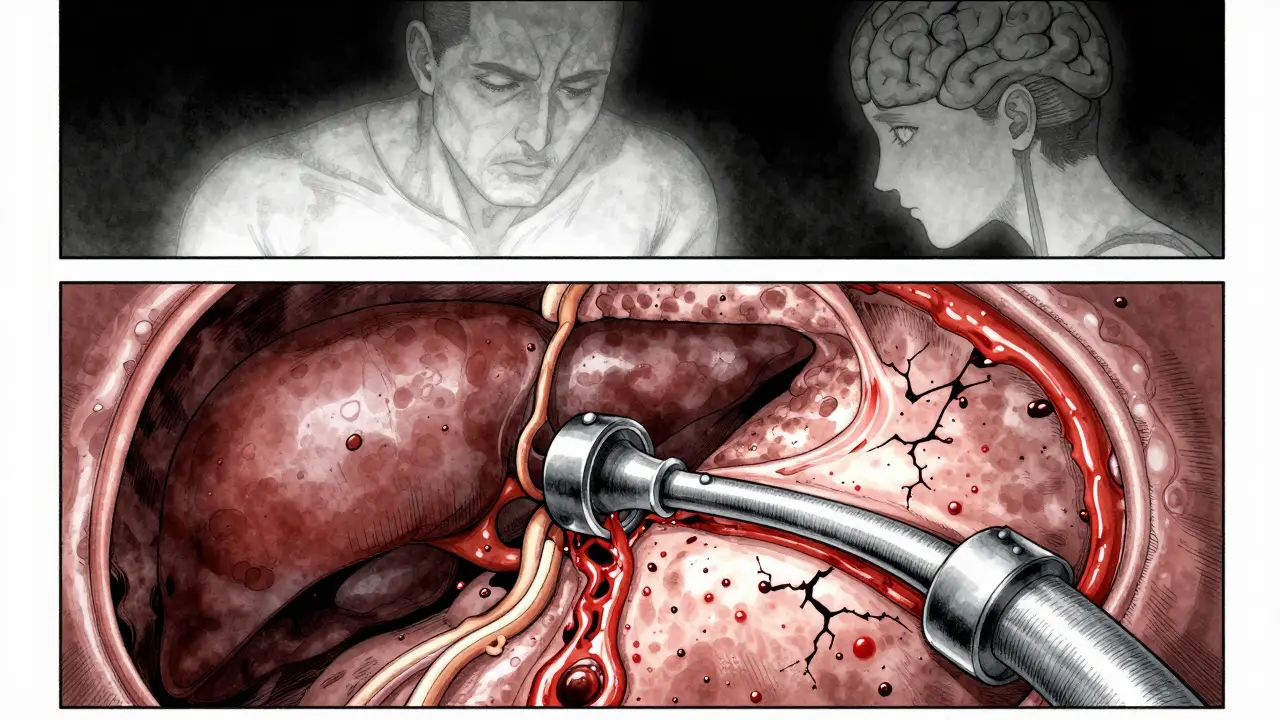
TIPS: A Bypass for the Liver
Think of TIPS - transjugular intrahepatic portosystemic shunt - as a metal stent tunnel built inside your liver. It connects the high-pressure portal vein to a low-pressure liver vein. Blood flows through the stent instead of trying to squeeze through scar tissue. Pressure drops. Ascites improves. Varices shrink. Success rates? 90-95% technical success. And for patients with refractory ascites, it’s often a game-changer. Seventy-eight percent report major quality-of-life improvements.
But there’s a catch. About 20-30% of patients develop hepatic encephalopathy after TIPS. That’s confusion, memory loss, slurred speech. Why? Because blood bypasses the liver. Toxins that should be filtered now flood the brain. It’s manageable with lactulose or rifaximin. But it’s a trade-off. TIPS isn’t for everyone. It’s reserved for those who’ve failed other treatments. And it requires a skilled interventional radiologist. You need at least 75 supervised procedures under your belt to do it safely.
Non-Cirrhotic Portal Hypertension: A Different Beast
Not everyone with portal hypertension has cirrhosis. About 10% don’t. Causes? Portal vein clots, schistosomiasis, or rare conditions like nodular regenerative hyperplasia. The treatment? Totally different. Beta-blockers? Useless here. Anticoagulation is key. Blood thinners like warfarin or direct oral anticoagulants, aiming for an INR of 2 to 3. The goal? Prevent the clot from growing and let the body re-route blood naturally. Missing this difference can be dangerous. Treating a clot like cirrhosis? It won’t work.
The Human Cost: More Than Numbers
Behind every statistic is a person. One patient on a liver forum said, “After my third paracentesis, I quit my job. I couldn’t stand for more than 20 minutes.” Another wrote, “The terror of vomiting liters of blood… I still wake up scared.” These aren’t just symptoms. They’re life-altering.
Quality of life scores for people with portal hypertension complications are 35-40 points lower than healthy peers. That’s like carrying a heavy backpack every day. Sleep is broken. Work is lost. Social life fades. Even the treatments have downsides. Beta-blockers cause fatigue. Paracentesis is invasive. TIPS can mess with your mind. No one talks enough about this emotional toll. But it’s real. And it’s part of managing the disease.
What’s Next? New Hope on the Horizon
The field is changing fast. In 2023, the FDA approved the Hepatica SmartBand - a wearable device that estimates portal pressure without a needle. It’s not perfect - 82% accuracy - but it could replace invasive HVPG measurements for many. Meanwhile, AI models are getting better at predicting who’s at risk of bleeding. Mayo Clinic’s model hits 92% accuracy.
Drugs are coming too. Simtuzumab, a monoclonal antibody targeting liver scarring, showed a 35% drop in portal pressure in phase 3 trials. It’s not approved yet, but it’s a breakthrough. And the big picture? Non-alcoholic fatty liver disease (NAFLD) is exploding. It’s now behind 24% of cirrhosis cases globally. That means more portal hypertension ahead. We need better, less invasive tools - and faster access to transplants. Right now, the average wait in the U.S. is 14 months.
What You Need to Do Now
- If you have cirrhosis: Get screened for varices with endoscopy. Don’t wait for bleeding.
- If you have ascites: Cut sodium. Take diuretics as prescribed. Track your weight daily - gain of 2 kg in a week? Call your doctor.
- If you’ve bled: Stay on beta-blockers and banding. Never skip follow-ups.
- If your fluid won’t drain: Ask about TIPS. It’s not a last resort - it’s a tool.
- If you’re not sure: Ask for an HVPG measurement. It’s the only way to know how bad your pressure really is.
Portal hypertension isn’t curable - yet. But it’s manageable. And with the right steps, you can live longer, avoid emergencies, and keep your life intact.
Can portal hypertension be cured?
No, portal hypertension itself cannot be cured unless the underlying liver damage is reversed - which rarely happens. The goal of treatment is to lower pressure, prevent complications like bleeding or fluid buildup, and improve survival. Liver transplant is the only potential cure, but it’s reserved for advanced cases. For most, management is lifelong.
How do I know if I have portal hypertension?
You usually don’t feel it until complications appear - bleeding, ascites, or confusion. But if you have cirrhosis or chronic liver disease, your doctor should screen you. Endoscopy checks for varices. Ultrasound or elastography can estimate pressure. The only definitive test is HVPG measurement - a procedure where a catheter is inserted into a liver vein to measure pressure directly. It’s not routine for everyone, but it’s the gold standard.
Are beta-blockers safe for everyone with portal hypertension?
Not always. People with asthma, very low blood pressure, heart failure, or slow heart rates may not tolerate them. Side effects like fatigue, dizziness, and cold hands are common. If you can’t take beta-blockers, endoscopic band ligation is the alternative. Your doctor will weigh risks and benefits. Never stop them suddenly - it can trigger dangerous bleeding.
What’s the difference between ascites and portal hypertension?
Portal hypertension is the high pressure in the liver’s blood vessels. Ascites is one of its complications - the fluid that leaks into the belly because of that pressure. Think of it this way: portal hypertension is the cause. Ascites is the symptom. You can have portal hypertension without ascites. But if you have ascites from liver disease, you almost certainly have portal hypertension.
Can diet alone manage ascites?
Diet is critical - sodium restriction under 2,000 mg/day is the foundation. But diet alone rarely controls ascites once it’s moderate to severe. Diuretics are almost always needed. For some, paracentesis or TIPS becomes necessary. Think of diet as the base layer - not the whole solution.
How often should I get screened for varices if I have cirrhosis?
If you have cirrhosis and no varices, get an endoscopy every 2 years. If you have small varices, repeat every 1 to 2 years. If you’ve had a bleed, you’ll need endoscopy every 1-2 years for banding, plus lifelong medication. Don’t skip these - varices can grow silently.
Janelle Pearl
March 7, 2026 AT 22:58Just read this whole thing through and honestly? I’m in tears. Not because it’s scary, but because someone finally put into words what living with this feels like. The fatigue, the isolation, the way your body betrays you - it’s all real. And nobody talks about how hard it is to keep going when every appointment feels like a countdown.
I’ve been managing ascites for 3 years. Weight checks. Diuretics. Salt-free meals that taste like cardboard. And still, some weeks, I wake up feeling like I’m wearing a water balloon as a suit. But I’m here. And if you’re reading this? You’re not alone.
Thank you for writing this. It matters more than you know.
Dan Mayer
March 8, 2026 AT 16:10Umm okay so first off the article says 'portal hypertension' is caused by cirrhosis but what about ALL the other causes like portal vein thrombosis?? Like why is everyone acting like cirrhosis is the only game in town?? This is why people die - because docs don’t even know the basics anymore.
Also 'beta blockers lower HR by 25%'? That’s not even accurate - it’s based on HVPG reduction, not heart rate. And who the heck is measuring HR like it’s a Fitbit? This is why medicine is broken.
Ray Foret Jr.
March 10, 2026 AT 08:59Man I just got diagnosed last month and this post saved me. Seriously. I was about to give up until I read the part about TIPS. I didn’t even know that was an option. My doc just said ‘drink less water’ and handed me a pamphlet.
So yeah… thanks for this. I’m gonna ask for an HVPG now. And maybe banding. And maybe a hug. 😊
Samantha Fierro
March 11, 2026 AT 21:37As a nurse who works in hepatology, I want to commend the depth and accuracy of this post. The distinction between cirrhotic and non-cirrhotic portal hypertension is critical - and so often overlooked.
I’ve seen patients denied TIPS because they were deemed ‘too young’ or ‘not sick enough.’ This isn’t just clinical - it’s ethical. We need to shift from reactive care to proactive management. Early screening saves lives.
Also - yes, diet matters. But no, it’s not enough. Please, if you’re reading this and you’re a provider - listen to your patients. Their weight gain isn’t ‘just water.’ It’s a warning.
Robert Bliss
March 12, 2026 AT 22:59lol i had no idea this was even a thing. my uncle had cirrhosis and i thought he just needed to stop drinking. turns out there’s a whole science behind it.
so beta blockers are like… a shield? and the bands are like… little rubber bands? that’s wild. i’m gonna share this with my family. thanks for making it simple.
Peter Kovac
March 14, 2026 AT 16:59The article is dangerously oversimplified. The claim that ‘90-95% technical success’ for TIPS equates to clinical success is misleading. Mortality within one year post-TIPS for refractory ascites is still 40-50%.
Furthermore, the assertion that AI models achieve ‘92% accuracy’ is based on retrospective datasets with selection bias. No prospective validation exists. This is not science - it’s marketing.
And the Hepatica SmartBand? 82% accuracy means 1 in 5 patients will receive incorrect management decisions. This is not innovation - it’s negligence dressed in tech.
APRIL HARRINGTON
March 15, 2026 AT 14:58Leon Hallal
March 15, 2026 AT 23:54Everyone’s acting like this is some new breakthrough. Newsflash - we’ve known about portal hypertension for 50 years. What’s new? The fact that we’re still letting people die because they can’t afford a transplant or can’t get a TIPS because their insurance says ‘no.’
This isn’t about medicine. It’s about money. And you’re all just dancing around the real issue.
Judith Manzano
March 17, 2026 AT 09:12This is so helpful. I’ve been wondering why my mom’s ascites keeps coming back even though she’s on spironolactone. The part about albumin replacement after paracentesis - I didn’t know that was standard. I’m going to bring this to her hepatologist tomorrow.
Also, the emotional toll section… that’s the part no one talks about. I didn’t realize how much her sleep loss and isolation were affecting her. Thank you for seeing the whole person.
rafeq khlo
March 18, 2026 AT 11:08It is imperative to note that the majority of the information presented herein is derived from American clinical guidelines, which are not universally applicable. In India, for instance, schistosomiasis remains a leading cause of non-cirrhotic portal hypertension, yet anticoagulation protocols are rarely implemented due to lack of infrastructure and physician awareness. Furthermore, the assertion that beta-blockers are contraindicated in asthma is outdated; selective beta-blockers such as nebivolol are now considered safe in mild-to-moderate cases. The article, while well-intentioned, perpetuates a Western-centric paradigm that neglects global epidemiological realities. This is not merely a clinical oversight - it is a systemic failure of medical education.